A .gov website belongs to an official government organization in the United States.
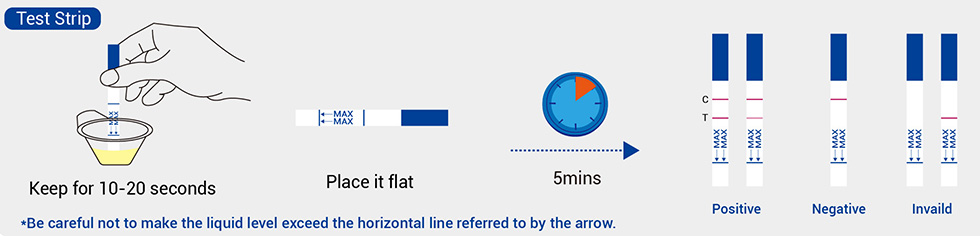
Secure .gov websites use HTTPS Respiratory Pathogen Testing Kit
A lock ( ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites.
The recommendations in this guidance continue to apply after the expiration of the federal COVID-19 Public Health Emergency.
For healthcare personnel, see Isolation and work restriction guidance. For strategies to mitigate healthcare personnel staffing shortages, see Contingency and crisis management. For healthcare professionals advising people in non-healthcare settings about isolation for laboratory-confirmed COVID-19, see Preventing Spread of Respiratory Viruses When You’re Sick.
This interim guidance has been updated based on currently available information about COVID-19 and the current situation in the United States. Updates were made to reflect the high levels of vaccine-and infection-induced immunity and the availability of effective treatments and prevention tools. This guidance provides a framework for facilities to implement select infection prevention and control practices (e.g., universal source control) based on their individual circumstances (e.g., levels of respiratory virus transmission in the community).
This guidance is applicable to all U.S. settings where healthcare is delivered (including nursing homes and home health). This guidance is not intended for non-healthcare settings (e.g., restaurants) and not for persons outside of healthcare settings. CDC’s main landing page for COVID-19 content will help readers navigate to information regarding modes of transmission, clinical management, laboratory settings, COVID-19 vaccines and CDC guidance on other COVID-19-related topics.
Employers should be aware that other local, territorial, tribal, state, and federal requirements may apply, including those promulgated by the Occupational Safety and Health Administration (OSHA).
With the end of the federal COVID-19 Public Health Emergency (PHE) on May 11, 2023, CDC will no longer receive data needed to publish Community Transmission levels for SARS-CoV-2. This metric informed CDC’s recommendations for broader use of source control in healthcare facilities to allow for earlier intervention, to avoid strain on a healthcare system, and to better protect individuals seeking care in these settings.
As described in CDC’s Core IPC Practices, source control remains an important intervention during periods of higher respiratory virus transmission. Without the Community Transmission metric, healthcare facilities should identify local metrics that could reflect increasing community respiratory viral activity to determine when broader use of source control in the facility might be warranted (See Appendix).
Encourage everyone to remain up to date with all recommended COVID-19 vaccine doses.
Establish a Process to Identify and Manage Individuals with Suspected or Confirmed SARS-CoV-2 Infection
Source control refers to use of respirators or well-fitting facemasks or cloth masks to cover a person’s mouth and nose to prevent spread of respiratory secretions when they are breathing, talking, sneezing, or coughing. Masks and respirators also offer varying levels of protection to the wearer. Further information about types of masks and respirators, including those that meet standards and the degree of protection offered to the wearer, is available at: Masks and Respirators. People, particularly those at high risk for severe illness, should wear the most protective mask or respirator they can that fits well and that they will wear consistently.
Even when a facility does not require masking for source control, it should allow individuals to use a mask or respirator based on personal preference, informed by their perceived level of risk for infection based on their recent activities (e.g., attending crowded indoor gatherings with poor ventilation) and their potential for developing severe disease if they are exposed.
Source control options for HCP include:
When used solely for source control, any of the options listed above could be used for an entire shift unless they become soiled, damaged, or hard to breathe through. If they are used during the care of patient for which a NIOSH Approved respirator or facemask is indicated for personal protective equipment (PPE) (e.g., NIOSH Approved particulate respirators with N95 filters or higher during the care of a patient with SARS-CoV-2 infection, facemask during a surgical procedure or during care of a patient on Droplet Precautions), they should be removed and discarded after the patient care encounter and a new one should be donned.
Source control is recommended for individuals in healthcare settings who:
Source control is recommended more broadly as described in CDC’s Core IPC Practices in the following circumstances:
Implement Universal Use of Personal Protective Equipment for HCP
If SARS-CoV-2 infection is not suspected in a patient presenting for care (based on symptom and exposure history), HCP should follow Standard Precautions (and Transmission-Based Precautions if required based on the suspected diagnosis).
As SARS-CoV-2 transmission in the community increases, the potential for encountering asymptomatic or pre-symptomatic patients with SARS-CoV-2 infection also likely increases. In these circumstances, healthcare facilities should consider implementing broader use of respirators and eye protection by HCP during patient care encounters as described below.
NIOSH Approved particulate respirators with N95 filters or higher used for:
Optimize the Use of Engineering Controls and Indoor Air Quality
Create a Process to Respond to SARS-CoV-2 Exposures Among HCP and Others
Healthcare facilities should have a plan for how SARS-CoV-2 exposures in a healthcare facility will be investigated and managed and how contact tracing will be performed.
If healthcare-associated transmission is suspected or identified, facilities might consider expanded testing of HCP and patients as determined by the distribution and number of cases throughout the facility and ability to identify close contacts. For example, in an outpatient dialysis facility with an open treatment area, testing should ideally include all patients and HCP. Depending on testing resources available or the likelihood of healthcare-associated transmission, facilities may elect to initially expand testing only to HCP and patients on the affected units or departments, or a particular treatment schedule or shift, as opposed to the entire facility. If an expanded testing approach is taken and testing identifies additional infections, testing should be expanded more broadly. If possible, testing should be repeated every 3-7 days until no new cases are identified for at least 14 days.
Guidance for outbreak response in nursing homes is described in setting-specific considerations below.
Healthcare facilities responding to SARS-CoV-2 transmission within the facility should always notify and follow the recommendations of public health authorities.
The IPC recommendations described below (e.g., patient placement, recommended PPE) also apply to patients with symptoms of COVID-19 (even before results of diagnostic testing) and asymptomatic patients who have met the criteria for empiric Transmission-Based Precautions based on close contact with someone with SARS-CoV-2 infection. However, these patients should NOT be cohorted with patients with confirmed SARS-CoV-2 infection unless they are confirmed to have SARS-CoV-2 infection through testing.
Duration of Empiric Transmission-Based Precautions for Symptomatic Patients being Evaluated for SARS-CoV-2 infection
The decision to discontinue empiric Transmission-Based Precautions by excluding the diagnosis of current SARS-CoV-2 infection for a patient with symptoms of COVID-19 can be made based upon having negative results from at least one viral test.
If a patient suspected of having SARS-CoV-2 infection is never tested, the decision to discontinue Transmission-Based Precautions can be made based on time from symptom onset as described in the Isolation section below. Ultimately, clinical judgment and suspicion of SARS-CoV-2 infection determine whether to continue or discontinue empiric Transmission-Based Precautions.
Duration of Empiric Transmission-Based Precautions for Asymptomatic Patients following Close Contact with Someone with SARS-CoV-2 Infection
In general, asymptomatic patients do not require empiric use of Transmission-Based Precautions while being evaluated for SARS-CoV-2 following close contact with someone with SARS-CoV-2 infection. These patients should still wear source control and those who have not recovered from SARS-CoV-2 infection in the prior 30 days should be tested as described in the testing section.
Examples of when empiric Transmission-Based Precautions following close contact may be considered include:
Patients placed in empiric Transmission-Based Precautions based on close contact with someone with SARS-CoV-2 infection should be maintained in Transmission-Based Precautions for the following time periods.
Duration of Transmission-Based Precautions for Patients with SARS-CoV-2 Infection
The following are criteria to determine when Transmission-Based Precautions could be discontinued for patients with SARS-CoV-2 infection and are influenced by severity of symptoms and presence of immunocompromising conditions. Patients should self-monitor and seek re-evaluation if symptoms recur or worsen. If symptoms recur (e.g., rebound), these patients should be placed back into isolation until they again meet the healthcare criteria below to discontinue Transmission-Based Precautions for SARS-CoV-2 infection unless an alternative diagnosis is identified.
In general, patients who are hospitalized for SARS-CoV-2 infection should be maintained in Transmission-Based Precautions for the time period described for patients with severe to critical illness.
In general, patients should continue to wear source control until symptoms resolve or, for those who never developed symptoms, until they meet the criteria to end isolation below. Then they should revert to usual facility source control policies for patients.
Patients with mild to moderate illness who are not moderately to severely immunocompromised:
Patients who were asymptomatic throughout their infection and are not moderately to severely immunocompromised:
Patients with severe to critical illness and who are not moderately to severely immunocompromised:
The exact criteria that determine which patients will shed replication-competent virus for longer periods are not known. Disease severity factors and the presence of immunocompromising conditions should be considered when determining the appropriate duration for specific patients. For a summary of the literature, refer to Preventing Spread of Respiratory Viruses When You’re Sick
Patients who are moderately to severely immunocompromised may produce replication-competent virus beyond 20 days after symptom onset or, for those who were asymptomatic throughout their infection, the date of their first positive viral test.
The criteria for the test-based strategy are:
Patients who are not symptomatic:
In addition to the recommendations described in the guidance above, here are additional considerations for the settings listed below.
Additional Guidance for Use of Isolation Gowns
Cleaning and Disinfecting Dialysis Stations
Considerations for vehicle configuration when transporting a patient with suspected or confirmed SARS-CoV-2 infection
Additional considerations when performing AGPs on patients with suspected or confirmed SARS-CoV-2 infection:
In general, long-term care settings (excluding nursing homes) whose staff provide non-skilled personal care* similar to that provided by family members in the home (e.g., many assisted livings, group homes), should follow community prevention strategies based on COVID-19 hospital admission levels, similar to independent living, retirement communities or other non-healthcare congregate settings. Residents should also be counseled about strategies to protect themselves and others , including recommendations for source control if they are immunocompromised or at high risk for severe disease. CDC has information and resources for older adults and for people with disabilities .
Visiting or shared healthcare personnel who enter the setting to provide healthcare to one or more residents (e.g., physical therapy, wound care, intravenous injections, or catheter care provided by home health agency nurses) should follow the healthcare IPC recommendations in this guidance. In addition, if staff in a residential care setting are providing in-person services for a resident with SARS-CoV-2 infection, they should be familiar with recommended IPC practices to protect themselves and others from potential exposures including the hand hygiene, personal protective equipment and cleaning and disinfection practices outlined in this guidance.
*Non-skilled personal care consists of any non-medical care that can reasonably and safely be provided by non-licensed caregivers, such as help with daily activities like bathing and dressing; it may also include the kind of health-related care that most people do themselves, like taking oral medications. In some cases where care is received at home or a residential setting, care can also include help with household duties such as cooking and laundry.
Use of well-fitting masks in healthcare settings are an important strategy to prevent the spread of respiratory viruses. Well-fitting masks can help block virus particles from reaching the nose and mouth of the wearer (wearer protection) and, if someone is ill, help block virus particles coming out of their nose and mouth from reaching others (source control). Masking by healthcare personnel as part of Standard and Transmission-Based Precautions and by ill individuals as part of respiratory hygiene and cough etiquette (i.e., for people with symptoms) are already well-described. This appendix describes considerations for implementing broader use of masking in healthcare settings. However, even when masking is not required by the facility, individuals should continue using a mask or respirator based on personal preference, informed by their perceived level of risk for infection based on their recent activities (e.g., attending crowded indoor gatherings with poor ventilation) and their potential for developing severe disease if they are exposed.
When to Implement Broader Use of Masking
The overall benefit of broader masking is likely to be the greatest for patients at higher risk for severe outcomes from respiratory virus infection and during periods of high respiratory virus transmission in the community.
Facilities should consider several factors when determining how and when to implement broader mask use:
Metrics for Community Respiratory Virus Transmission
CDC is in the early stages of developing metrics that could be used to guide when to implement select infection prevention and control practices for multiple respiratory viruses. However, at this time there are some general metrics that could be used to help facilities make decisions about community respiratory virus incidence. Data on the exact metric thresholds that correspond with a higher risk for transmission are lacking. In addition, data from these systems are generally not available for all jurisdictions.
Some facilities might consider recommending masking during the typical respiratory virus season (approximately October-April).
Facilities could also follow national data on trends of several respiratory viruses.
Healthcare Personnel (HCP): HCP refers to all paid and unpaid persons serving in healthcare settings who have the potential for direct or indirect exposure to patients or infectious materials, including body substances (e.g., blood, tissue, and specific body fluids); contaminated medical supplies, devices, and equipment; contaminated environmental surfaces; or contaminated air. HCP include, but are not limited to, emergency medical service personnel, nurses, nursing assistants, home healthcare personnel, physicians, technicians, therapists, phlebotomists, pharmacists, dental healthcare personnel, students and trainees, contractual staff not employed by the healthcare facility, and persons not directly involved in patient care, but who could be exposed to infectious agents that can be transmitted in the healthcare setting (e.g., clerical, dietary, environmental services, laundry, security, engineering and facilities management, administrative, billing, and volunteer personnel).
Healthcare settings refers to places where healthcare is delivered and includes, but is not limited to, acute care facilities, long-term acute-care facilities, nursing homes, home healthcare, vehicles where healthcare is delivered (e.g., mobile clinics), and outpatient facilities, such as dialysis centers, physician offices, dental offices, and others.
Source control: Use of respirators, well-fitting facemasks, or well-fitting cloth masks to cover a person’s mouth and nose to prevent spread of respiratory secretions when they are breathing, talking, sneezing, or coughing. Source control devices should not be placed on children under age 2, anyone who cannot wear one safely, such as someone who has a disability or an underlying medical condition that precludes wearing one safely, or anyone who is unconscious, incapacitated, or otherwise unable to remove their source control device without assistance. Face shields alone are not recommended for source control. At a minimum, source control devices should be changed if they become visibly soiled, damaged, or hard to breathe through. Further information about source control options is available at: Masks and Respirators (cdc.gov)
Cloth mask: Textile (cloth) covers that are intended primarily for source control in the community. They are not personal protective equipment (PPE) appropriate for use by healthcare personnel. Guidance on design, use, and maintenance of cloth masks is available.
Facemask: OSHA defines facemasks as “a surgical, medical procedure, dental, or isolation mask that is FDA-cleared, authorized by an FDA EUA, or offered or distributed as described in an FDA enforcement policy. Facemasks may also be referred to as ‘medical procedure masks’.” Facemasks should be used according to product labeling and local, state, and federal requirements. FDA-cleared surgical masks are designed to protect against splashes and sprays and are prioritized for use when such exposures are anticipated, including surgical procedures. Other facemasks, such as some procedure masks, which are typically used for isolation purposes, may not provide protection against splashes and sprays.
Respirator: A respirator is a personal protective device that is worn on the face, covers at least the nose and mouth, and is used to reduce the wearer’s risk of inhaling hazardous airborne particles (including dust particles and infectious agents), gases, or vapors. Respirators are approved by CDC/NIOSH, including those intended for use in healthcare.
Airborne Infection Isolation Rooms (AIIRs):
Immunocompromised: For the purposes of this guidance, moderate to severely immunocompromising conditions include, but might not be limited to, those defined in the Interim Clinical Considerations for Use of COVID-19 Vaccines
Close contact: Being within 6 feet for a cumulative total of 15 minutes or more over a 24-hour period with someone with SARS-CoV-2 infection.
SARS-CoV-2 Illness Severity Criteria (adapted from the NIH COVID-19 Treatment Guidelines)
The studies used to inform this guidance did not clearly define “severe” or “critical” illness. This guidance has taken a conservative approach to define these categories. Although not developed to inform decisions about duration of Transmission-Based Precautions, the definitions in the National Institutes of Health (NIH) COVID-19 Treatment Guideline s are one option for defining severity of illness categories. The highest level of illness severity experienced by the patient at any point in their clinical course should be used when determining the duration of Transmission-Based Precautions. Clinical judgment regarding the contribution of SARS-CoV-2 to clinical severity might also be necessary when applying these criteria to inform infection control decisions.
Mild Illness: Individuals who have any of the various signs and symptoms of COVID-19 (e.g., fever, cough, sore throat, malaise, headache, muscle pain) without shortness of breath, dyspnea, or abnormal chest imaging.
Moderate Illness: Individuals who have evidence of lower respiratory disease by clinical assessment or imaging, and a saturation of oxygen (SpO2) ≥94% on room air at sea level.
Severe Illness: Individuals who have respiratory frequency >30 breaths per minute, SpO2 <94% on room air at sea level (or, for patients with chronic hypoxemia, a decrease from baseline of >3%), ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) <300 mmHg, or lung infiltrates >50%.
Critical Illness: Individuals who have respiratory failure, septic shock, and/or multiple organ dysfunction.
In pediatric patients, radiographic abnormalities are common and, for the most part, should not be used as the sole criteria to define COVID-19 illness category. Normal values for respiratory rate also vary with age in children, thus hypoxia should be the primary criterion to define severe illness, especially in younger children.
In situations where the use of a respirator is not required either by the employer or by an Occupational Safety and Health Administration (OSHA) standard, the employer may still offer filtering facepiece respirators or permit employees to use their own respirators as long as the employer determines that such respirator use will not in itself create a hazard. This is considered voluntary use under the Respiratory Protection Standard . CDC encourages employers to permit workers to voluntarily use filtering facepiece respirators like N95s. If an employer allows voluntary use of filtering facepiece respirators, the employer must provide users with 29 CFR 1910.134 Appendix D – Information for Employees Using Respirators When Not Required Under the Standard. See 29 CFR 1910.134(c)(2) for additional requirements applicable to voluntary respirator use.
Healthcare personnel, both paid and unpaid, should be allowed to bring their own highly protective masks (such as N95 respirators) as long as the mask does not violate the facility’s safety and health requirements. They should not be asked to remove their more protective source control device (a well-fitting N95 respirator, for example) for a less protective device (such as a procedure mask) unless the mask or respirator is visibly soiled, damaged, or hard to breathe through. However, devices brought from home may not be appropriate for protecting healthcare personnel from all job hazards, and they should change to recommended personal protective equipment when indicated (for instance, before entering the room of a patient managed with Transmission-Based Precautions). Learn more about the types of masks and respirators and infection control recommendations for healthcare personnel.
CDC recommends that people visiting healthcare facilities use the most protective form of source control (masks or respirators) that fits well and will be worn consistently. Healthcare facilities may choose to offer well-fitting facemasks as a source control option for visitors but should allow the use of a clean mask or respirator with higher level protection by people who chose that option based on their individual preference. Masks and respirators used for source control should be changed if they become visibly soiled, damaged, or hard to breathe through. Learn more about the types of masks and respirators and infection control recommendations for healthcare personnel.
CDC’s guidance to use NIOSH-approved particulate respirators with N95 filters or higher when providing care for patients with suspected or confirmed SARS-CoV-2 infection is based on the current understanding of SARS-CoV-2 and related respiratory viruses.
Facemasks commonly used during surgical procedures will provide barrier protection against droplet sprays contacting mucous membranes of the nose and mouth, but they are not designed to protect wearers from inhaling small particles. NIOSH-approved particulate respirators with N95 filters or higher, such as other disposable filtering facepiece respirators, powered air-purifying respirators (PAPRs), and elastomeric respirators, provide both barrier and respiratory protection because of their fit and filtration characteristics.
Respirators should be used as part of a respiratory protection program that provides staff with medical evaluations, training, and fit testing.
Although facemasks are routinely used for the care of patients with common viral respiratory infections, NIOSH-approved particulate respirators with N95 filters or higher are routinely recommended for emerging pathogens like SARS CoV-2, which have the potential for transmission via small particles, the ability to cause severe infections, and limited or no treatment options. While the situation is evolving for SARS-CoV-2, CDC continues to recommend respiratory protection while the impact of new variants is being assessed.
In general, transport and movement of a patient with suspected or confirmed SARS-CoV-2 infection outside of their room should be limited to medically essential purposes. If being transported outside of the room, such as to radiology, healthcare personnel (HCP) in the receiving area should be notified in advance of transporting the patient. For transport, the patient should wear a well-fitting source control (if tolerated) to contain secretions and their body should be covered with a clean sheet.
If transport personnel must prepare the patient for transport (e.g., transfer them to the wheelchair or gurney), transport personnel should wear all recommended PPE (gloves, a gown, a NIOSH-approved particulate respirator with N95 filters or higher, and eye protection [i.e., goggles or disposable face shield that covers the front and sides of the face]). This is recommended because these interactions typically involve close, often face-to-face, contact with the patient in an enclosed space (e.g., patient room). Once the patient has been transferred to the wheelchair or gurney (and prior to exiting the room), transporters should remove their gown and gloves and perform hand hygiene.
The transporter should continue to wear their respirator. The transporter should also continue to use eye protection if there is potential that the patient might not be able to tolerate their well-fitting source control device for the duration of transport. Additional PPE should not be required unless there is an anticipated need to provide medical assistance during transport (e.g., helping the patient replace a dislodged facemask).
After arrival at their destination, receiving personnel (e.g., in radiology) and the transporter (if assisting with transfer) should perform hand hygiene and wear all recommended PPE. If still wearing their original respirator and eye protection, the transporter should take care to avoid self-contamination when donning the remainder of the recommended PPE. This cautious approach will be refined and updated as more information becomes available and as response needs change in the United States.
EMS personnel should wear all recommended PPE because they are providing direct medical care and are in close contact with the patient for longer periods of time.
In general, minimize the number of personnel entering the room of patients who have SARS-CoV-2 infection. Healthcare facilities should consider assigning daily cleaning and disinfection of high-touch surfaces to nursing personnel who will already be in the room providing care to the patient. If this responsibility is assigned to EVS personnel, they should wear all recommended PPE when in the room. PPE should be removed upon leaving the room, immediately followed by performance of hand hygiene.
After discharge, terminal cleaning can be performed by EVS personnel. If not wearing all recommended PPE, they should delay entry into the room until time has elapsed for enough air changes to remove potentially infectious particles. After this time has elapsed, EVS personnel can enter the room and should wear a gown and gloves when performing terminal cleaning; well-fitting source control might also be recommended. Eye protection and a facemask (if not already worn for source control) should be added if splashes or sprays during cleaning and disinfection activities are anticipated or otherwise required based on the selected cleaning products. Shoe covers are not recommended at this time for SARS-CoV-2.
Some procedures performed on patients are more likely to generate higher concentrations of infectious respiratory aerosols than coughing, sneezing, talking, or breathing. These aerosol generating procedures (AGPs) potentially put healthcare personnel and others at an increased risk for pathogen exposure and infection.
Development of a comprehensive list of AGPs for healthcare settings has not been possible, due to limitations in available data on which procedures may generate potentially infectious aerosols and the challenges in determining if reported transmissions during AGPs are due to aerosols or other exposures.
There is neither expert consensus, nor sufficient supporting data, to create a definitive and comprehensive list of AGPs for healthcare settings.
Commonly performed medical procedures that are often considered AGPs, or that might create uncontrolled respiratory secretions, include:
Based on limited available data, it is uncertain whether aerosols generated from some procedures may be infectious, such as:
*Aerosols generated by nebulizers are derived from medication in the nebulizer. It is uncertain whether potential associations between performing this common procedure and increased risk of infection might be due to aerosols generated by the procedure or due to increased contact between those administering the nebulized medication and infected patients.
References related to aerosol generating procedures:
Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J (2012) Aerosol Generating Procedures and Risk of Transmission of Acute Respiratory Infections to Healthcare Workers: A Systematic Review. PLoS ONE 7(4); https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3338532/#!po=72.2222external iconexternal icon ).
The amount of time that the air inside an examination room remains potentially infectious depends on a number of factors including the size of the room, the number of air changes per hour, how long the patient was in the room, if the patient was coughing or sneezing, and if an aerosol-generating procedure was performed.
In general, it is recommended to restrict HCP and patients without PPE from entering the room until sufficient time has elapsed for enough air changes to remove potentially infectious particles.
General guidance is available on clearance rates under differing ventilation conditions.
In addition to ensuring sufficient time for enough air changes to remove potentially infectious particles, HCP should clean and disinfect environmental surfaces and shared equipment before the room is used for another patient.
Preprocedural mouth rinses (PPMR) with an antimicrobial product (e.g. chlorhexidine gluconate, povidone-iodine) have been shown to reduce the level of oral microorganisms in aerosols and spatter generated during dental procedures. Evidence from recent studies suggest that some PPMR solutions are efficacious and may temporarily decrease the viral load of SARS-CoV-2 in the oral cavity. Targeted clinical studies are currently underway to learn more about the potential role of PPMR and the prevention of SARS-CoV-2 transmission.
Because more research is needed to demonstrate the effectiveness of PPMR in preventing transmission of SARS-CoV-2 in the dental setting, CDC does not provide a recommendation for or against the use of PPMR before dental procedures. However, if PPMR are used before dental procedures, they should be used as an adjunct to other infection prevention and control measures recommended to decrease the spread of infectious diseases in dental settings. Such measures include delaying elective dental procedures for patients with suspected or confirmed SARS-CoV-2 infection until they are no longer infectious or for patients who meet criteria for quarantine until they complete quarantine.
Due to concerns about increased transmissibility of the SARS-CoV-2 Omicron variant, this guidance is being updated to enhance protection for healthcare personnel, patients, and visitors and to address concerns about potential impacts on the healthcare system given a surge in SARS-CoV-2 infections. These updates will be refined as additional information becomes available to inform recommended actions.
N95 and NIOSH Approved are certification marks of the U.S. Department of Health and Human Services (HHS) registered in the United States and several international jurisdictions.
Hpv Test 16 18 To receive email updates about COVID-19, enter your email address: